
September 2023 Case
Background
The neuropathology of brain tumors consists of several different entities; however, brain metastases from primary cancers are the most common type. Approximately 98,000 to 170,000 metastatic brain tumor cases occur each year in the United States1. Some primary cancers are more commonly found to migrate to the brain, such as lung, breast, and melanoma, whereas others are rarely to be discovered there. Cancer cells pass through the bloodstream and into the central nervous system through the blood-brain barrier. These cells then continue to proliferate, invade, and can show different patterns of distribution. Carcinoma brain metastases present macroscopically as well demarcated lesions, and microscopically as cohesive clusters or sheets of cells, most often identified solely on morphology. Here, we present a case of a lung primary carcinoma that has a unique infiltrative, single cell pattern morphology.
Clinical History
We report a 50–60-year-old patient with a history of stage IV, non-small cell lung carcinoma that has metastasized to the bone, brain, uterus, and adrenals, with a RET fusion by next-generation sequencing (NGS). The brain metastasis was complicated by left facial paralysis and obstruction hydrocephalus. Patient was originally treated with selpercatinib, a craniotomy and ventriculostomy, and whole brain radiation therapy (WBRT). The patient’s radiation treatment was complicated by respiratory failure and severe dysphagia, requiring a percutaneous endoscopic gastrotomy (PEG) tube. Patient also has a perforated left corneal ulcer, in which a transplant was conducted.
On magnetic resonance imaging (MRI) of the brain, progression of 2 areas concerning for recurrent disease versus radiation effect with mild surrounding edema in the right and left cerebellum was seen. The patient was treated with stereotactic radiosurgery (SRS), in which a follow-up MRI showed tumor regression. Most recent MRI brain showed increased enhancement and edema especially in the right frontal and right occipital regions (Figure 1).
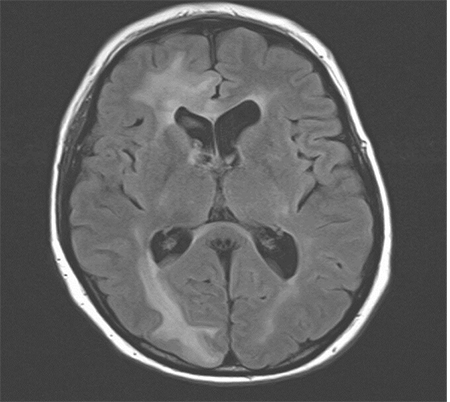
Figure 1. Magnetic resonance imaging (MRI). Sagittal view of edematous lesions representing metastatic carcinoma in the right frontal and occipital regions
A biopsy of the right frontal brain was conducted, in which sections showed a highly unusual phenomenon of individual, perivascular cell infiltrate of the white matter and cortex (Figure 2). These lesional cells stain positive for keratin and TTF-1 and are morphologically identical to the patient’s prior solid tumor (Figure 2). The patient then underwent a right frontal craniotomy.
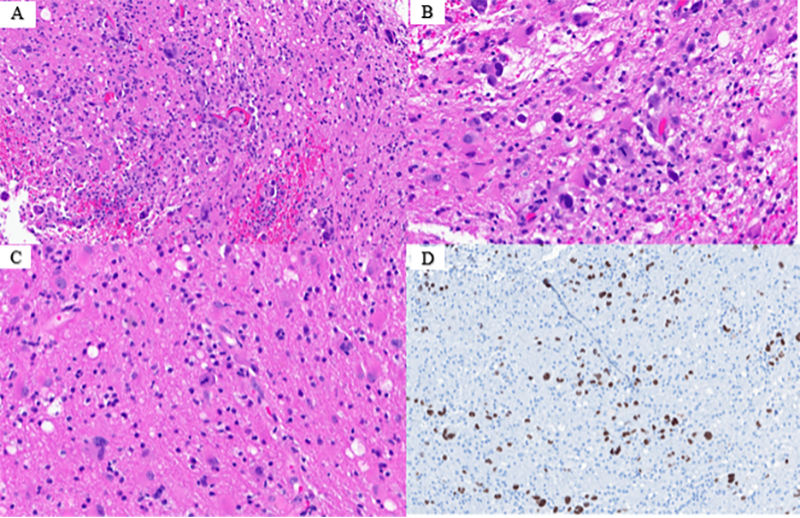
Figure 2. Metastatic primary non-small cell lung carcinoma. A. Single cell infiltration of tumor cells within the white matter and cortex of the brain (4X) B. Single cell infiltration of tumor cells within the white matter and cortex of the brain (10X) C. Single cell infiltration of tumor cells
Discussion
Lung cancer is the most common malignancy to metastasize to the brain and has the highest mortality rate, emphasizing the importance of early detection and targeted early-stage of disease treatment2. Cell migration has shown to play a pivotal role in the oncogenesis of early lung cancer, in which cancer cells cross normal epithelial cells prior to invasion3. In non-small cell lung cancers, TP53 mutations are the most common. TP53 can increase cell migration by its regulation of Rho-GTPase. Studies have suggested targeting Rho-GTPase can slow the progression of early non-small cell lung cancer3. There has also been investigation into cellular origin of the drivers of migration in lung cancer cells. A previous study (Wang, Zihao, et al., 2023) found subclones of primary tumor with a gain of chromosome 7 played a role in the migration of brain metastasis, and potential targeted therapy of brain metastasis-associated epithelial cells (BMAECs) was identified4.
Oncogenic driver alterations have become an interest to identifying targeted treatment regimens in non-small cell lung cancer. The therapeutic impact has been shown to improve the outcome in these patients, however, data involving each biomarker is limited5,6. The importance of these biomarkers also puts emphasis on the early detection and screening of lung cancer, particularly stage I lung tumors2,3,6. Molecular classification, outcome and aggression prediction, and potential adjuvant treatments are ways to improve the current clinical course of disease. Recent studies have shown particular importance on the molecular mutation EGFR, and the improvement when treated with osimertinib6.
The cohesion of tumor cells and its involvement in crossing the blood-brain barrier in carcinomas has been studied in breast cancers. Brain microvascular endothelial cells (BMECs) and breast carcinoma tumor cells were used and analyzed in an environment recreating shear stress. The interaction of these cells was found to compromise the blood-brain barrier. This was shown by the separation of junctional proteins, β-catenin and zonula occludens-1, resulting in permeability. Both cell types revealed alterations in connexin 43, which is a vital gap junction protein. This allowed breast cancer tumors cells to obtain migratory characteristics7.
Lung cancers and melanoma are most associated with multiple metastases in the brain, which is representative in this case. Non-small cell carcinoma is most often found to have multiple foci, around blood vessels, without parenchymal invasion8. Macroscopically, brain metastasis are sharply demarcated, round tumors that cause mass effect and edema, but do not infiltrate the surrounding tissue8. Microscopically, tumors show morphology similar to primary tumors, and the surrounding parenchyma often shows gliosis, which represents the edema seen on imaging8. However, we presented a patient with very rare histologic morphology demonstrating metastatic carcinoma to the brain, with a pattern of infiltration via individual tumor cells. Metastatic carcinoma to the brain does not have the tendency to infiltrate, and it is almost always found in clusters. The mass effect and edema seen in this case is consistent with imaging findings typically seen in non-small cell lung carcinoma metastases; however, the infiltrative, single cell features seen histologically are a common feature of high-grade gliomas, or primary central nervous system tumors, and not characteristic of carcinoma.
References
- Amsbaugh MJ, Kim CS. Brain Metastasis. [Updated 2023 Apr 3]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-.
- Zhang R, Xia Y, Wang Z, Zheng J, Chen Y, Li X, Wang Y, Ming H. Serum long non coding RNA MALAT-1 protected by exosomes is up-regulated and promotes cell proliferation and migration in non-small cell lung cancer. Biochem Biophys Res Commun. 2017 Aug 19;490(2):406-414.
- Millar FR, Janes SM, Giangreco A. Epithelial cell migration as a potential therapeutic target in early lung cancer. Eur Respir Rev. 2017 Jan 31;26(143):160069.
- Wang Z, Wang Y, Chang M, Wang Y, Liu P, Wu J, Wang G, Tang X, Hui X, Liu P, Guo X, Xing B, Wang Y, Han Z, Ma W. Single-cell transcriptomic analyses provide insights into the cellular origins and drivers of brain metastasis from lung adenocarcinoma. Neuro Oncol. 2023 Jul 6;25(7):1262-1274.
- Rodríguez M, Ajona D, Seijo LM, Sanz J, Valencia K, Corral J, Mesa-Guzmán M, Pío R, Calvo A, Lozano MD, Zulueta JJ, Montuenga LM. Molecular biomarkers in early stage lung cancer. Transl Lung Cancer Res. 2021 Feb;10(2):1165-1185.
- Godinho-Pereira J, Garcia AR, Figueira I, Malhó R, Brito MA. Behind Brain Metastases Formation: Cellular and Molecular Alterations and Blood-Brain Barrier Disruption. Int J Mol Sci. 2021 Jun 30;22(13):7057.
- Pekmezci M, Perry A. Neuropathology of brain metastases. Surg Neurol Int. 2013 May 2;4(Suppl 4):S245-55.